2020
A Patients Guide to Health Equity, Partnership and Collaboration
Of the more than 200 different types of cancers, breast cancer remains the most common. It is important to note that breast cancer does not affect all men and women the same. Even living in North America, unfortunately still impacts their access to care. As researchers work to address disparities it remains critical to look at communities at the grassroots level. Tigerlily Foundation and American Association for Cancer Research (AACR) hosted a special session at the 2020 San Antonio Breast Cancer Symposium that addressed the importance of health, collaboration and partnership with Black, Indigenous and people of color (BIPOC). The numerous research studies shared during our special sessions suggest that the primary reasons for breast cancer-related health disparities are rooted in large part by socio-economic differences. However, even the most educated and economically advantaged Black, Indigenous and persons of color (BIPOC) have a higher prognosis of cancer compared to White women. Tigerlily Foundation is committed to working with medical researchers and professionals to address racial and socio-economic disparities in breast cancer care. Sharing these findings with you, as an advocate and ally, is part of our mission to end disparities – of age, stage and color, in our lifetime.
Where You Live Impacts Your Cancer Survival
The University of Miami and Florida International University are the first to use a new measure, the Index of Concentration at the Extremes (ICE), to analyze the effects of economics and the neighborhood you live in (racial/ethnic residential segregation) on breast cancer survival in South Florida. The study looked at 6,145 breast cancer patients from South Florida.
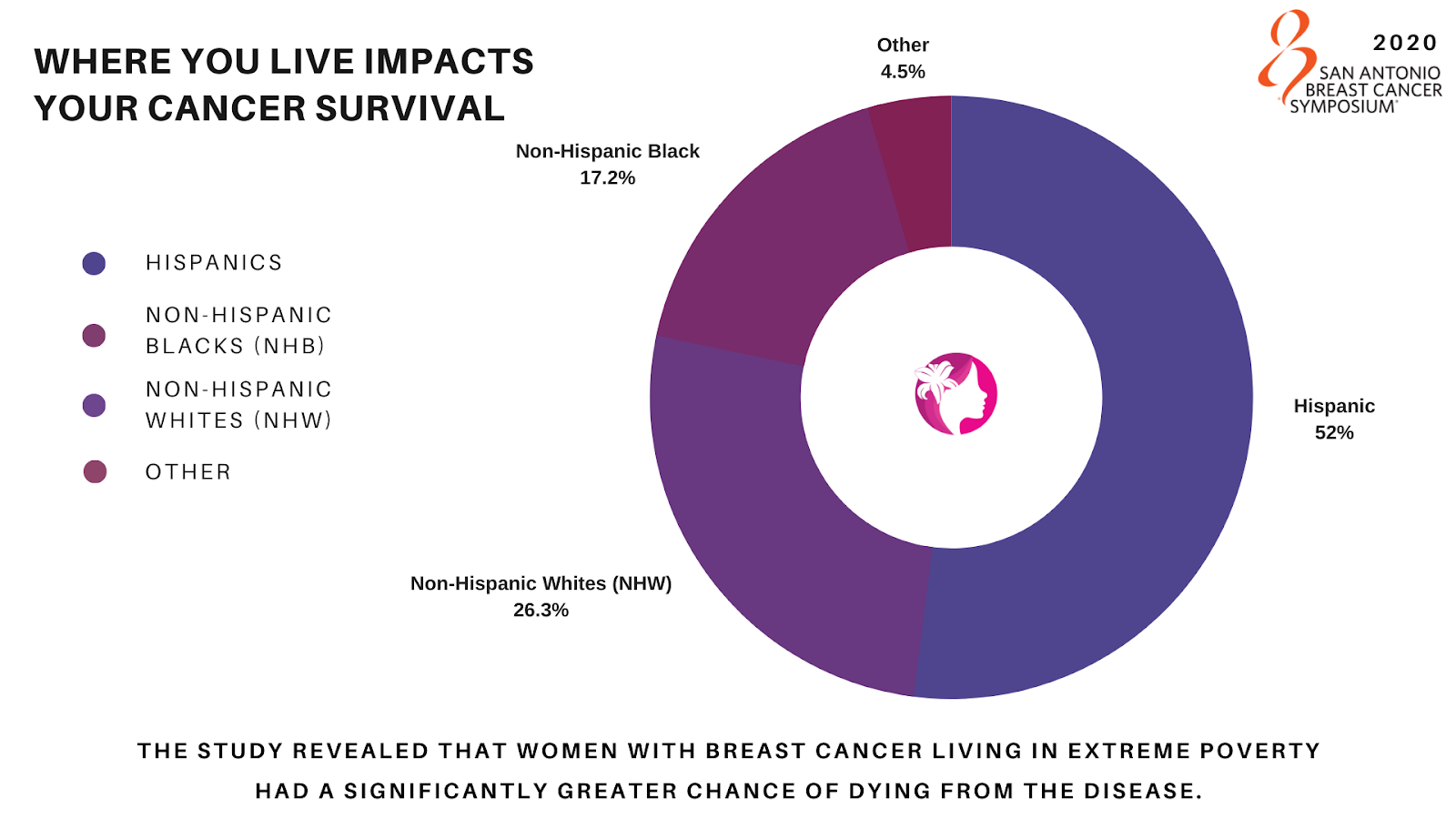
With over 52% Hispanic, 26.3% Non-Hispanic Whites (NHW), and 17.2% Non-Hispanic Blacks (NHB) represented, the study revealed that women with breast cancer living in extreme poverty had a significantly greater chance of dying from the disease.
In conclusion, The University of Miami and Florida International University found that breast cancer survival disparities are partly influenced by extreme racial/ethnic residential and economic segregation. When accounting for socio-demographics, tumor characteristics, the guideline for appropriate treatment from the National Comprehensive Cancer Network (NCCN), disparities remained. This suggests potential social and environmental factors that impact survival. Further supporting the need for effective interventions that account for the social and environmental contexts in which cancer patients live and are treated.
Tigerlily Foundation’s Points to Consider:
- Are there any other studies like this happening anywhere else in the United States?
- What will be the impact COVID-19 has on the already overwhelmed health care system in underserved communities that work with and serve individuals in extreme poverty?
Where you live matters: Impact of economic, racial/ethnic, and racialized economic residential segregation on breast cancer survival – Goel N, Kelly KN, Yadegarynia S, Choi S, Kesmodel SB, Westrick A. University of Miami, Miami, FL; Florida International University, Miami, FL.
Racial Disparities in Breast Cancer Screening
In another study by Johns Hopkins University in Baltimore, Maryland they assessed 140,346 women between 2013-2020. Researchers tracked breast cancer screening methods, focusing on racial differences in utilization and effectiveness. The use of Digital Breast Tomosynthesis (DBT), a more effective screening technique compared to traditional two-dimensional digital mammography (FFDM), rapidly increased over the study period, however, Black and Asian women were less likely to have had a screening with DBT compared to White women.
Racial disparities persist despite with uptake of digital breast tomosynthesis (DBT) for breast cancer screening – Ambinder EB, Oluyemi E, Visvanathan K. Johns Hopkins, Baltimore, MD
Tigerlily Foundation’s Points to Consider:
- While screening rates between Black and White women are similar, the modalities of screening vary. Research data shows that healthcare is segregated, possibly driven by racial differences in sites of care.
- DBT is not offered widely. The detection advantage of DBT vs. FFDM is most prominent for women with dense breasts. There is evidence that Black and Asian women have more dense breasts than White women, if age and body mass index (BMI) are adjusted in the study.
- We would like to understand if the patients were able to access 3D mammograms without a referral from their healthcare provider? Is access based on availability or non-referrals?
Reducing Racial Disparities in Oncoplastic Surgery
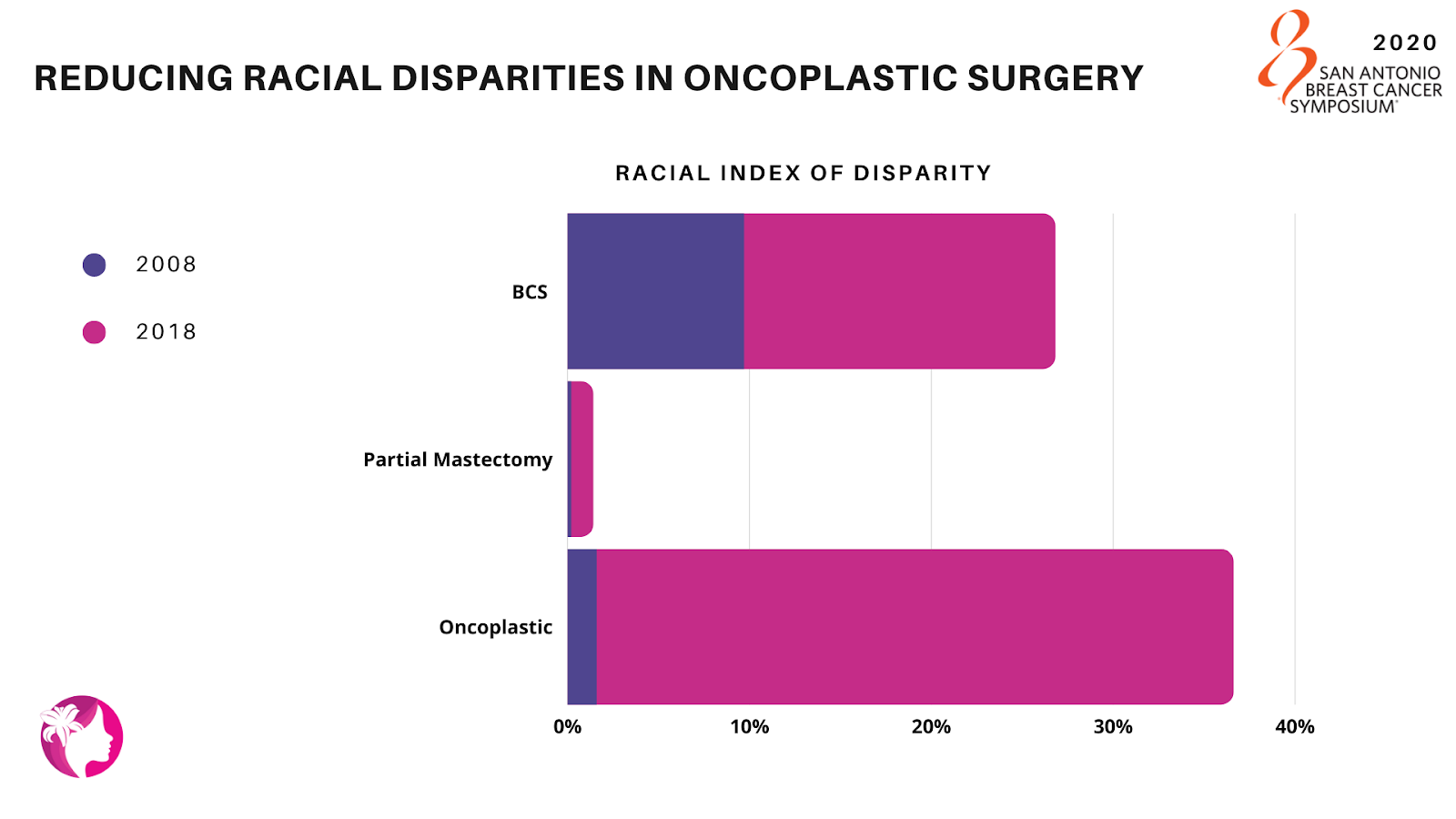
Here is a study from the National Surgical Quality Improvement Program (NSQIP) looking at 180,700 women who underwent Breast Conservation Surgery (BCS). They identified through the database between 2008-2018, racial differences in BCS utilization rates (partial mastectomy and oncoplastic/reconstructive surgery) that were examined to determine how the rates changed over the period of time. Of the 46% of women who underwent BCS, 92% underwent a partial mastectomy and 8% received oncoplastic procedures.
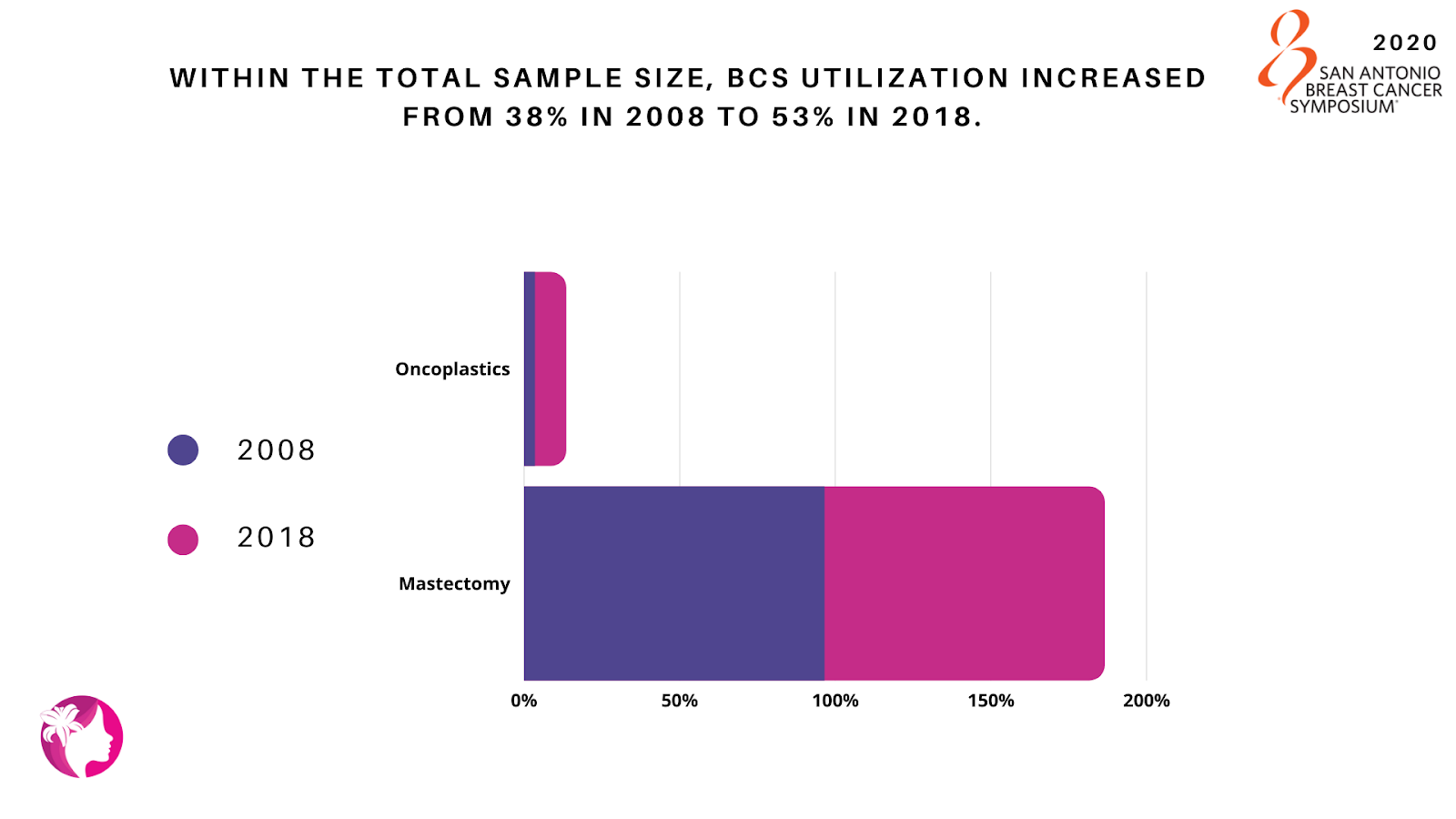
The proportion of patients having oncoplastics increased from 3.5% in 2008 to 10% in 2018, leading to a declining proportion of partial mastectomies: 96.5% to 90.0%. Overall, oncoplastic utilization between 2008 and 2018 increased from 4% to 10% in Asian and White patients, and 1% to 10% in Black patients.
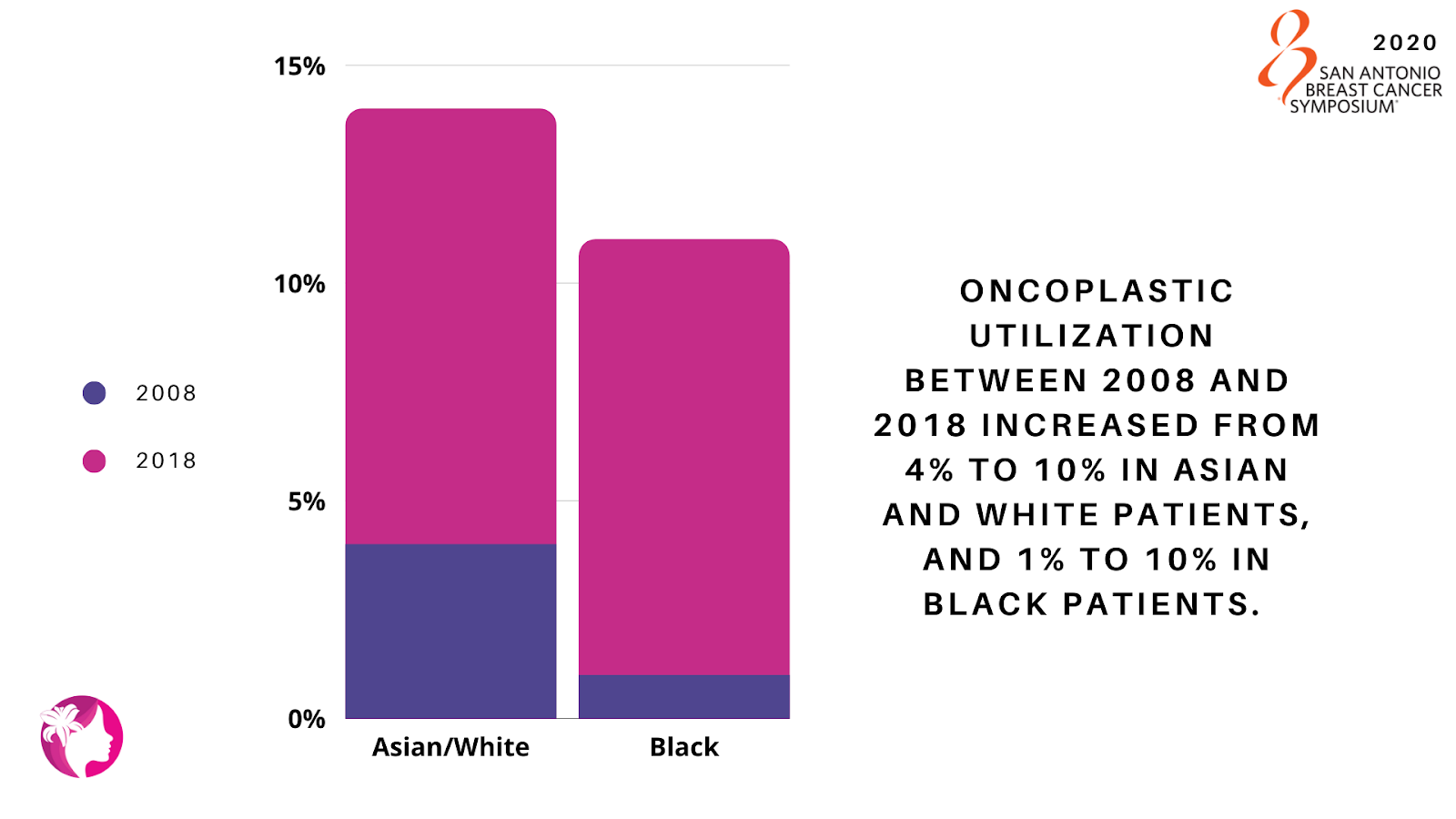
The racial index of disparity for BCS patients decreased from 17.1% to 9.7%; while the index of disparity has remained relatively unchanged for partial mastectomies (1.2% to 0.2%), but significantly decreased in oncoplastics (35% to 1.6%) indicating an improvement in racial disparities for oncoplastic procedures. This study demonstrates promising progress within the field of breast conservation surgery with a decreasing index of disparity among races especially in oncoplastic surgery.
Examining a decade of racial disparity in partial mastectomy and oncoplastic surgery – Jean J, Jonczyk MM, Homsy C, Naber S, Chatterjee A. Tufts University School of Medicine, Boston, MA; Tufts Medical Center, Boston, MA.
Tigerlily Foundation’s Points to Consider:
- What caused a significant decrease of racial disparities in oncoplastics but not partial mastectomies?
- Was information and options provided by the patients’ health care provider?
- Were regional differences apparent for mastectomy and partial mastectomy rates?
Triple-Negative Breast Cancer Rates Higher Among African-Ancestry Patients
Research indicates that African-Ancestry (AA) patients experience a disproportionately higher rate of Triple-Negative Breast Cancer (TNBC) than European-Ancestry (EA) patients.
The University of Chicago performed a study on genomic and transcriptomic sequencing of breast tumors comparing 221 AA and 341 EA patients at the molecular level. While the biological drivers behind this disparity remain unknown between ancestral populations, EA TNBC patients in comparison to AA TNBC patients exhibited higher mutation rates in certain tumors such as BRCA2, HR-/HER2+ and FGF3.
The study’s results concluded that there were significant differences in breast tumor heterogeneity and mutation spectrum in TNBC and HR+/HER2- breast cancers between AA and EA patients. Additionally, ancestral differences were also observed in the activity of relevant signaling pathways for TNBC. Overall, the results identify previously unexplored pathways and molecular phenotypes of aggressive disease, providing opportunities for development of more effective biomarker informed treatment of breast cancer in diverse populations.
More comprehensive research and case studies need to be implemented on African-Ancestry (AA) patients. Not having this understanding of how the disease impacts AA patients, it can become more aggressive and causes a higher mortality rate.
Comprehensive genomic and transcriptomic profiling of molecular subtypes reveal ancestral differences in the activity of signaling pathways between patients with African and European ancestry – Miyashita M, Bell JSK, Zheng Y, Yoshimatsu T, Rajagopal PD, Woodard A, Reynier JB, Sveen E, Khramtsova G, Liu F, Ibraheem A, Fleming G, Jaskowiak N, Nanda R, Leibowitz B, Beaubier N, White K, Huo D, Olopade OI. The University of Chicago, Chicago, IL; Tempus Inc, Chicago, IL.
Tigerlily Foundation’s Points to Consider:
- How do we encourage the scientific community to create more clinical trials that address genomic and transcriptomic sequencing?
- How do we support access and patient confidence in clinical trials, in particular ensuring that we have enough patients in African-Ancestry?
Racial Differences in Breast Cancer Immune Microenvironments
The rate of mortality among Black women is 40% higher than among White women. Although, the cause of this staggering difference is still not completely understood, a growing body of evidence leads scientists to take a closer look at the immune microenvironment (the interaction between cancer cells and other cells within and around a tumor) to find answers.
The authors used the Carolina Breast Cancer Study (CBCS), a large population-based study, and a test they created to identify 48-genes from 13 immune cell types in 1,957 breast cancer patients, including 53% Black and 47% non-Black women. The study identified three breast cancer phenotypes defined by the level of activity of the immune microenvironment which correlated to risk of recurrence, intrinsic subtype, age and race. Immune response differences may be targetable to improve treatment response, and therefore it is important to identify race- and subtype-specific differences in immune microenvironments as these are the two most notable differences in this study.
Racial differences in breast cancer immune microenvironments – Hamilton AM, Olsson LT, Calhoun BC, Hoadley KA, Troester MA. University of North Carolina at Chapel Hill, Chapel Hill, NC.
Tigerlily Foundation’s Points to Consider:
- How can we tailor cancer treatment specific to race sub-type and immune microenvironments?
Racial Disparities in long-term Survival after Chemotherapy
Pathological complete response (pCR) is a strong predictor of long-term survival among breast cancer patients who receive chemotherapy before undergoing surgery. pCR occurs when the tissue no longer contains any cancer cells after treatment with chemotherapy then surgery. In a study by the University of Chicago, they looked at 595 stage I-III breast cancer patients. Researchers sought to determine whether racial disparity existed in the rate of pCR. The results of the study showed that significantly fewer Black patients achieved pCR than White patients.
Even after adjusting for tumor subtype and clinical stage, Black patients still had a much lower chance of achieving pCR after neoadjuvant chemotherapy. While the delayed initiation of treatment might have partially contributed to the racial disparity, black women with hormone receptor negative, HER2 positive breast cancer had the largest disparity.
Researchers concluded additional investigation is required as this study was quite small.
Racial disparities in pathological complete response among breast cancer patients receiving neoadjuvant chemotherapy – Zhao F, Steiner M, Ibraheem A, Fleming G, Jaskowiak N, Nanda R, Olopade OI, Huo D. University of Chicago, Chicago, IL.
Tigerlily Foundation’s Point to Consider:
- Clinical trial involvement should be encouraged within the Black community. On average, Black women do not have complete pathologic responses to neoadjuvant chemo, which reemphasizes the inherent biological differences Blacks have in response to available therapeutics.
Did you know Gene Expression Differs Between West African and East African Breast Tumors?
Global frequency of triple-negative breast cancer (TNBC) reveals a unique pattern that suggests there may be genetic increased risk specific to TNBC.
In a recent study, West African and African-American women were associated with higher rates of TNBC than East African women and White American women. Even within TNBC cases, outcomes differ between race groups, which may be due to differences in TNBC subtypes/biology, related to genetic ancestry. The study sought to determine the difference in genetic expression and TNBC tumor environments in two distinct ways (race vs. ancestry). The study looked at Ghanaian (West African) and Ethiopian (East African) by analyzing gene expressions. Scientists found hundreds of genes differentially expressed in TNBC tumors between the two groups.
This important ground-breaking study is first of its kind and demonstrates the need for deeper research in African ancestry.
Martini R, Gebregzabher E, Dorsaint P, Chu T, Arora K, Gibbs L, Manojlovic Z, Robine N, Sboner A, Elemento O, Carpten J, Newman L, Davis M. Weill Cornell Medical College, New York City, NY; New York Genome Center, New York City, NY; University of Southern California, Los Angeles, CA.
Tigerlily Foundation’s Points to Consider:
- Tigerlily Foundation and its partners encourage and support further research and development in this area.
- Does the data vary by group based for all stages of disease (early-stage vs metastatic)? Is there a survival difference based on race or ancestry and the associated genes?
- The possible genetic variation between West and East African.
The Impact of Medicaid Expansion on the Gap between American Indians and Whites on Breast Cancer Management and Prognosis
Significant disparities in outcome exist between American Indian (Indigenous) and White populations. Between 1999 and 2009, breast cancer-related death rates did not decline significantly among American Indians (Indigenous) compared to Whites.
While insurance coverage undoubtedly plays a vital role in ensuring access to preventative services and breast cancer care, it is uncertain how this may affect patient outcomes. When the Affordable Care Act of 2010 rolled out the Medicaid Expansion, a larger percentage of the population gained access to health insurance coverage.
A group of researchers sought to determine how this expansion affected breast cancer management and prognosis for American Indians (Indigenous) compared to Whites. The study results were mixed. While early breast cancer diagnosis increased among American Indians (Indigenous), 3-year mortality rates did not change.
Tigerlily Foundation’s Points to Consider:
- Tigerlily Foundation and partners recognize the disparities in health care impacting the Indigenous population across the United States. It is not acceptable that the 3-year mortality rate did not change, even with greater access to Medicaid.
Did Medicaid expansion under the Affordable Care Act narrow the gap between American Indians and Whites on breast cancer management and prognosis? – Gaba AG, Cao L, Renfrew R, Egland KA, Witte DL, Wernisch J, Crosby R. Sanford Roger Maris Cancer Center, Fargo ND; Sanford Research, Fargo, ND; Sanford Health, Fargo, ND; SAb Biotherapeutics, Sioux Falls, SD; Sanford Research, Sioux Falls, SD; Sanford Center for Biobehavioral Research, Fargo, ND.
Impact of Medicaid Expansion on Breast Reconstruction in Low-Income Breast Cancer Patients
Researchers studied Ohio women (low income, 30–64-year-old, newly diagnosed) with local or regional spread of breast cancer in the post-Medicaid expansion between 2014-2016. This study was to determine whether the Time To initiation of Treatment (TTT) following a breast cancer diagnosis decreased. This research is important since significant delays in TTT can affect quality of life and increase mortality rates.
Using data from the Northeast Ohio Cancer Assessment and Surveillance Engine (NEO-CASE), researchers identified 30–64-year-old women with a new diagnosis of invasive, non-metastatic BC who were uninsured or on Medicaid when diagnosed, excluding women with incomes above 138% of Federal Poverty Level. Though no significant change in TTT was observed, the percentage of uninsured in the low-income group fell by more than half. The percent of women undergoing reconstructive surgery increased from the pre-to the post-Medicaid expansion period, a change not observed in the privately insured control group. Overall, TTT increased by 2 days post-expansion which is statistically insignificant.
Despite the lack of improvements in TTT, the study notes the drop in the percentage of uninsured BC patient’s post-expansion. They also noticed a decrease in the percentage of women diagnosed with regional-stage disease. Lastly, they noticed an increase in BC patients undergoing reconstruction. Taken together, these trends show an overall positive impact of Medicaid expansion on BC process of care and outcome measures.
Medicaid expansion associated with earlier stage and improved reconstruction rates in low income breast cancer patients – Rose J, Dong W, Kim U, Obeng-Gyasi S, Koroukian S. Case Western Reserve University, Cleveland, OH; Ohio State University Medical Center, Columbus, OH.
Tigerlily Foundation’s Points to Consider:
- Would the United States benefit from a healthcare system similar to Canada, Norway and Sweden?
- What would this cost and how would you implement it?
Impact of Medicaid Expansion on Racial Disparities and Initiation of Chemotherapy Treatment
When patients receive late adjuvant chemotherapy, the harder it is for the body to fight the disease even with medical intervention. There is a greater risk of the cancer spreading. Racial and ethnic minorities, uninsured populations, and low-income patients experience such delays far more often.
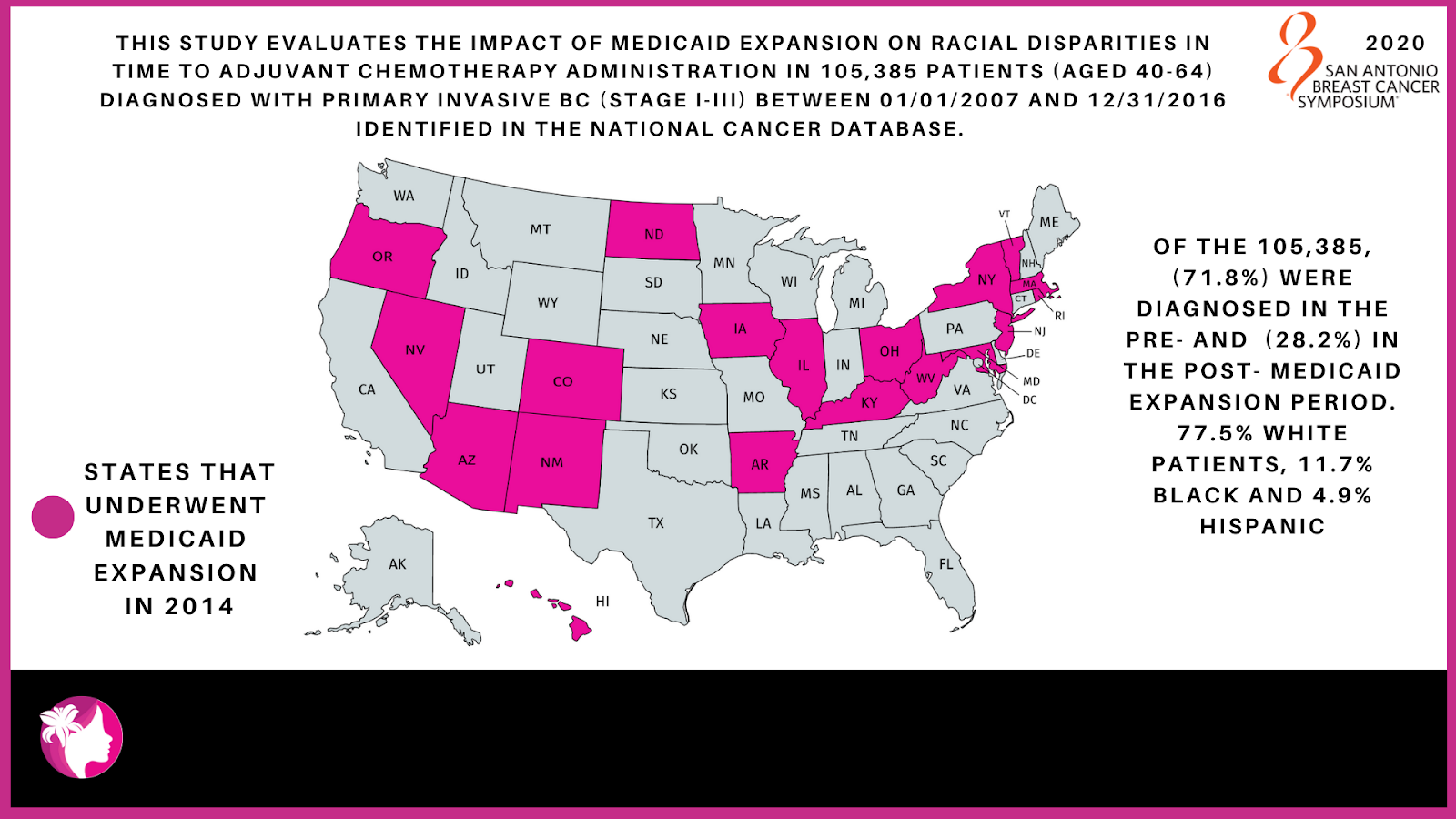
A provision in the Affordable Care Act called for expansion of Medicaid eligibility in order to cover more low-income Americans. This study evaluates the impact of Medicaid expansion on racial disparities in time to adjuvant chemotherapy administration. The study looked at 105,385 patients (aged 40-64) diagnosed with primary invasive BC (stage I-III) between 01/01/2007 and 12/31/2016 identified in the National Cancer Database.
Of the total sample size 71.8% (75,663) were diagnosed in the pre-Medicaid expansion period and 28.2% (29,722) in the post- Medicaid expansion period. The racial breakdown includes 77.5% White, 11.7% Black and 4.9% Hispanic patients. In both study periods Blacks and Hispanics experienced chemotherapy initiation delays compared to Whites. The proportion of chemotherapy delays decreased for all races between the pre- and the post-expansion period.
Researchers observed a statistically significant decrease in racial disparity in the chemotherapy initiation and demonstrated that Medicaid expansion reduced racial disparities. This in turn decreased the proportion of Blacks and Hispanics experiencing delays in adjuvant chemotherapy initiation and the gap that exists when compared to Whites.
Impact of Medicaid expansion on racial disparities in time to adjuvant chemotherapy administration among breast cancer (BC) patients Chavez-MacGregor M, Lei X, Zhao H, Shih T, Giordano SH. The University of Texas MD Anderson Cancer Center, Houston, TX.
Tigerlily Foundation’s Points to Consider:
- Many of the Southern states that have the largest Black populations chose not to expand Medicaid under the Affordable Care Act.
- 11 Million undocumented immigrants not covered by the Affordable Care Act.
How do Socioeconomic, Demographic, and Genomic Factors Affect Breast Cancer Mortality?
Studies have shown that health services, socio-demographic, clinical, and genomic factors all contribute to breast cancer disparities. The degree to which each factor contributes to health outcomes in cancer is uncertain.
In a retrospective study (a study of past data) used Formalin-Fixed Paraffin-Embedded (FFPE) breast cancer (BC) tissue collected between 1992-2006 within the Iowa and Hawaii (SEER Residual Tissue Repositories). Researchers created the first-in-kind linkage of SEER-Medicare data to physical tumor samples to combine clinical, health services, and genomic data into a single group. This linkage allows genomic analyses with clinical and health services data.
Researchers anticipate that this analysis method may offer new ways to explain links between biology, access, and disparities in breast cancer outcomes.
Comprehensive analysis of health services, sociodemographic, clinical, and genomic factors driving locally advanced breast cancer mortality via a first-in-kind linkage of SEER-Medicare data with physical tumor samples Robinson TJ, Wilson L, Marcom PK, Troester M, Lynch CF, Hernandez B, Castellar EP, Brauer HA, Enewold L, Dinan M. H. Lee Moffitt Cancer Center, Tampa, FL; Duke University Medical Center, Durham, NC; University North Carolina Chapel Hill, Chapel Hill, NC; University of Iowa, Des Moines, IA; University of Hawaii Cancer Center, Honolulu, HI; Gates Foundation, Seattle, WA; NIH, Bethesda, MD.
Tigerlily Foundation’s Points to Consider:
- How do encourage more industries and Key Opinion Leaders (KOL) to sign the #InclusionPledge and extending to our social and family networks to get involved.
This article was co-authored and peer reviewed by Erica Warner, ScD, MPH; Arnethea Sutton, Ph.D.; Onyinye D. Balogun, M.D., Melissa Davis, PhD; Ogori N. Kalu, MD, Maimah Karmo, Diana Porter Bodden, Shanda Cooper, MSc., Tania Koulakian and Jacqueline Seylmes.
What our ANGELs have to say
“I did enjoy the session. Although there is a long way to go to end disparities, it seems that studies and research are asking questions that will inform steps that can be taken to improve outcomes.”
“Much new evidence and research was presented, as well as new hypotheses and explanations offered for disparities.”
“The “voices” included were largely research studies or from clinicians. The information included was relevant and directly important to patients, but I didn’t feel like the patient voice was necessarily included.”
“I am aware that breast cancer outcomes might be improving, but significant disparities exist in that improvement. I felt this presentation was a hopeful step in getting to the root causes in order to eliminate these disparities. Changes in screening, treatment, access and understanding of tumor biology were all proposed. The field of social stressors, allostatic load, and social epigenetics were raised, but leave room for further investigation and discussion.”
Sound Therapy: The Power of the Voice
By: Michaela Bekenn
PART 2: The Power of the Voice
One of the most ancient tools for healing, used around the globe, is an instrument that is compact, inexpensive, and innate: the human voice. Let’s dive into practical tools that you can apply to create harmony from the inside out.
Go ahead and take a deep breath in, then let it out with a sigh or audible yawn. Perhaps create an elongated sound of “AH” on your exhale. This is not meant to be pretty. Instead this sound is one of active release. Try creating the open vowel “AH” a few more times, experimenting with volume, pitch (high/low sound) and duration. You might explore making different sounds one at a time such as “UH” “OOO” “EH” “EYE” “AUM” etc. Creating defined sounds in an intentional way with the voice is called vocal toning. It is important to release judgement, and see this as a fun experiment. Find out what feels good and natural for you!
What do you experience in your body when you engage your voice? How and where do you feel the sound vibration? Does it travel, does it seem isolated to one region? Perhaps try placing your hand upon the area of the chest or belly while making a sound. lf you turn your awareness inward, what sensations, both physical and emotional do you notice?
Using sound for therapeutic outcomes begins with setting an intention to be carried through the vibration. What are you looking to bring into your life today, what sentiment are you offering yourself or others? Care, attention, forgiveness, love?
Now gently begin to hum, by slightly pursing your lips and keeping your tongue to the upper palate. Focus on directing an “MMM” sound to the front of your face. From there you can direct the sound to different regions of the body. Perhaps to areas that feel tight or tense. There is no wrong way to do this. The voice is intuitive and wise all by itself. The first step is trusting what comes out naturally.
Now you might be wondering, where is the science-based evidence that proves using the voice in this way is effective? Here’s a fun fact: sound travels faster in water because the particles are more densely packed. When sound is made in water the liquid will often change shape and produce intricate patterns. The human body is made of about 60% water, therefore it naturally responds to the effects of sound and can literally reorganize itself based on the sound frequencies it absorbs.
When we hum and create sound through the voice, there are a long list of benefits. Think of the relaxation that can be achieved for those who like to receive massage therapy for aiding pain, tension, or injury. Humming is a vibrational massage for the organs, tissues, and cells!
Research proves that when someone is engaged with humming for prolonged periods (5 min or more) the following begins to take place:
- Increased oxygen to the blood, brain, and cells
- Lowered blood pressure and heart rate
- Reduced stress
- Activating the parasympathetic nervous system (responsible for rest & digest response)
- Release of oxytocin (hormone responsible for feelings of love, trust, and belonging)
- Increase of nitric oxide (neural transmitter that creates lymphatic circulation, boosts immune system, and relaxes the muscles)
- Release of endorphins (creates a lift in energy and blocks pain receptors)
- Production of melatonin (sleep hormone that aids relaxation, natural anti-aging and anti-inflammatory)
The list goes on! For further reading I highly recommend a book by leading pioneers in western sound medicine The Humming Effect by Jonathan Goldman and Andi Goldman found here.
The voice is a deeply personal and powerful tool. It is always there for you. Next time you find yourself in a stressful moment, perhaps tune into the sounds you can detect, take a breath, and begin to hum for a few minutes. Notice how quickly your energy shifts. Heightened emotions such as stress, fear, worry, can be soothed by being transformed into soundwaves. You could also make sound with the intention of projecting a vibration of love or peace out across the planet. Sound has the power to disperse your intention. Composer, sound therapist and researcher Steven Halpern said “sound is the carrier wave of consciousness.”
To deepen your journey of healing with sound, join me for a weekly self love sound bath hosted by Tigerlily Foundation. Enjoy the soothing vibrations of crystal singing bowls, chimes, guitar and more, while experimenting with simple vocal toning and humming exercises. May you stay curious, and unleash the healing benefits of sound through the power of your own voice!
Check out Michaela’s weekly Sound Bath Thursdays at 7pm on Zoom. Register Here: https://www.tigerlilyfoundation.org/programs/support/pure-cat-initiative/
Sound Therapy: what is it and how does it function in everyday life?

By: Michaela Bekenn
PART 1: Sound as a Tool for Healing, Harmony, and Wellbeing
As a singer-songwriter and certified sound therapy practitioner, my work is centered around the power of sound and its impact on the physical, mental, emotional, and energetic body.
Sound is an ancient form of medicine, used for centuries to support wellbeing and accompany various stages of life. In what ways can sound be therapeutic and why is the human body sensitive to sound? Certain frequencies have been proven to create lasting benefits when applied with intention, including reducing stress, soothing pain, releasing emotional stagnation, improving sleep, boosting immunity, and encouraging cellular rejuvenation. How does this research relate to your own life? Think of a time when music shifted the energy of a moment. Perhaps at a ceremony, a concert, or at home during this pandemic. How were you supported or affected by the sound in your environment? Sound can have both a subtle and monumental impact on one’s mood, physiological responses, and sense of connection with others.
If you tune in right now: what can you hear or what vibration can you feel? There is likely a symphony of sound surrounding you, which can easily be drowned out by the noise of thoughts. So take a moment, take a breath, maybe close your eyes and begin to listen in a deeper way. Perhaps you can sense the singing of birds, the movement of traffic, another human voice, or the low hum of a nearby appliance.
Many people think of music as being made exclusively by those who identify as musicians. Perhaps they even go as far as declaring, “I am not musical.” And yet, every human being is born with the innate gift of sound, vibration, and rhythm. The first thing that a child does when they arrive into the world is make sound through crying. Vibration is a primary mode of communication for the infant and parents alike. Secondly, each of us carries around an inner drum that sustains us at all times. You guessed it, the heart. From a musical perspective, the heart is like a metronome, a natural keeper of time. The heart helps all the other organs function in a cohesive and mutually rhythmic way.
Science proves that everything that is in motion has a vibration. Therefore, every tissue, bone, and cell in the human body emits its own unique vibration and frequency. The brain is part of this equation too! The neural pathways communicate by sending messages through small electrical pulses. Essentially, the human body is a living breathing symphony. Music is often defined as “organized sound” and the body is one of the most organized instruments out there! So if you still don’t believe that you are musical, linger a while longer.
When it comes to health and wellbeing, just as an instrument can go out of tune, so can the human body. When the body is functioning with mental, physical, and emotional equilibrium harmony is achieved. In an orchestra when one instrument is playing out of tune, something begins to sound “off,” which is called dissonance. The same is true for the human body. Inner dissonance occurs when a particular region is not functioning in balance with the whole. This disharmony can result in fatigue, pain, discomfort, and illness. Sound and the use of the voice can be a primary tool in helping to restore and preserve the natural state of harmony required for rejuvenation and healing. Think of it as re-tuning the body, mind, and spirit. When we look at the current research as well as personal accounts of the effects of sound on holistic health, it is not surprising that Albert Einstein predicted, “Medicine of the future will be the medicine of frequencies.” The field of sound therapy is ancient and yet there is still so much to uncover.
Keep an eye out for next week’s blog focused on the power of the voice and the many ways you can engage your inner instrument to ignite balance and harmony in your life.
Experience a Sound Bath LIVE with Michaela every Thursday at 7pm on Zoom. Click here to register.
Dont Throw Away Your Confidence
Author: Katherine Couvillon
Last week, I took a new fitness class via Zoom. It was a special offering for breast cancer patients and survivors. At the end of the class, the instructor offered some words of encouragement for us. He reminded us of what we’d all been through – the devastating diagnosis, the grief, the pain, the doing of hard things, the chemo, the recovery, the scars. Each one of us had come through all of that, and he wanted to remind us of the strength we had had to endure it. He urged us to build on that, not to forget about or throw away what had been hard-earned through our cancer ordeals, that we should have confidence in our future abilities because of what we’d already survived.
With the words, “Don’t throw away,” my mind immediately jumped to Hebrews 10:35-36, which starts with, “So do not throw away your confidence.” I had memorized those verses through a song as a child but had never really thought about what they meant beyond the reference to perseverance. In their entirety, they read, “So do not throw away your confidence; it will be richly rewarded. You need to persevere so that when you have done the will of God, you will receive what He has promised” (NIV).
This concept of having confidence to face trials wasn’t new to me. Whenever I share my testimony, I share how God’s movement in my life through my divorce and years alone revealed His character to me and demonstrated that I could, in fact, go through things I would never have imagined I could survive – in His strength. And that once you’ve seen God faithfully carry you through something awful, you have confidence later that He will carry you through the next thing. I face cancer with less fear than I might have because I saw Him work so mightily in me through these other trials.
But apparently I didn’t need to learn all that from personal experience. I could have just read the verses right before those in the song I was so familiar with.
Remember those earlier days after you had received the light, when you endured in a great conflict full of suffering. Sometimes you were publicly exposed to insult and persecution; at other times you stood side by side with those who were so treated. You suffered along with those in prison and joyfully accepted the confiscation of your property, because you knew that you yourselves had better and lasting possessions. So do not throw away your confidence; it will be richly rewarded. You need to persevere so that when you have done the will of God, you will receive what he has promised (Heb. 10: 32-36).
Hebrews says: Remember your suffering and how God carried you through. Let that inform the future suffering you encounter. Don’t throw away your confidence; let it embolden you. You can do all things through Christ. Even this. God will carry you through once again. And He will even reward you if you persevere. Win-win.
Metastatic Bone Disease (MBD) and Breast Cancer
What is Metastatic Bone Disease?
The bones are one of the most common sites for breast cancer to spread, and when the cancer spreads to the bones, it’s called Metastatic Bone Disease (MBD), or bone metastases.3 Although cancer has spread to the bones, it is not considered bone cancer since the cancer didn’t originate in the bones. Breast cancer can spread to any bone, but the most common sites are the ribs, spine, pelvis, and long bones in the arms and legs.4
MBD is considered a common, but very serious complication of breast cancer that puts patients at risk for skeletal complications called skeletal-related events (SREs). These events can reduce quality of life and increase medical costs and risk of death.
What are the Risk Factors for MBD? Researchers have discovered risk factors that contribute to MBD, including:
- Gender: MBD occurs in both men and women but is particularly common in women with breast cancer.
- Age: MBD does not typically occur until after the age of 40.
- Cancer History: A person living with cancer, or with a family history of cancer, is at higher risk for developing MBD. However, MBD can be diagnosed in people without personal or familial history of cancer.
Symptoms of MBD
People who have MBD often experience pain as their first symptom, but there are other associated symptoms, including:
- Fractures (pathological bone fractures): Weakened bones can cause fractures resulting from a fall or injury, but also from everyday activities. Pathological bone fractures, however, are caused by disease. Typically occurring in the long bones of the arms and legs, they can cause severe pain.
- Constipation, nausea, loss of appetite: When calcium from the bones is released into the bloodstream, it can cause constipation, nausea, loss of appetite, confused or altered mental state and severe thirst.9 High blood calcium levels, also called hypercalcemia, can increase urine production, leading to dehydration, weakness and fatigue.6
- Spinal cord compression: Increased growth of cancer in the spine can press against the spinal cord and cause compression of the nerves, leading to numbness and weakness in the lower area of the body, pain or stiffness in the neck, back or lower back, paralysis, trouble with urinating and a lack of bowel movements.
Diagnosing MBD
Depending on the location and severity of the pain, MBD can be diagnosed by:
- X-Ray or Radiography
- Bone scans
- Bone biopsies
- CT (computer tomography) scans
- MRI (magnetic resonance imaging)
- PET (positron emission tomography)
- Blood tests measuring elevated levels of alkaline phosphatase (an enzyme that originates in the bone) and calcium levels to confirm hypercalcemia
Treatment Options for MBD6
If you are diagnosed with MBD, the primary goal of treatment is preventing SRE’s as they can significantly impact quality of life. Treatment options that are clinically proven include:
- Bone therapies, which involve using a bone-targeting agent, a class of drugs that prevent the loss of bone density by reducing the turnover of bone. There are various types of agents or medications (e.g. pills, intravenously) that can reduce fractures and slow the spread of cancer, which is dependent on the individual disease.12
- Anti-cancer therapies, such as chemotherapy, immunotherapy and hormone therapy, are systemic treatments that affect the whole body. While they are not specifically aimed at MBD, they may be used as a part of a treatment plan.
- Local treatments can be targeted to one specific area of the body. These types of local treatments can include:
- Radiation, a nonsurgical option which kills the cancer cells, helps to relieve pain, slow tumor growth and prevent bone breakage.
- Surgery, which is performed to remove the tumor and fix the broken or weakened bone in place using instruments such as wires, plates, rods or bone cement, which is used to strengthen or stabilize the bone.
MBD Infographic – Click here to download
References:
- Coleman, Robert. Skeletal Complications of Malignancy. Suppl Cancer. American Cancer Society Journal. https://acsjournals.onlinelibrary.wiley.com/doi/pdf/10.1002/%28SICI%291097-0142%2819971015%2980%3A8%2B%3C1588%3A%3AAID-CNCR9%3E3.0.CO%3B2-G. Accessed October 19, 2020.
- National Institutes of Health. Osteoporosis and African American Women. https://www.bones.nih.gov/health-info/bone/osteoporosis/background/african-american-women. Accessed October 19, 2020.
- Susan G Komen. Bone Metastases and Metastatic Breast Cancer. https://ww5.komen.org/BreastCancer/BoneMetastasesAndMetastaticBC.html. Accessed October 19, 2020.
- BreastCancer.org. Bone Metastasis: Symptoms and Diagnosis. https://www.breastcancer.org/symptoms/types/recur_metast/metastic/bone. Accessed October 19, 2020.
- So, Alan et al. Management of skeletal-related events in patients with advanced prostate cancer and bone metastases: Incorporating new agents into clinical practice. Can Urol Assoc J. 2012 Dec; 6(6): 465–470. PMID: 23282666.
- American Academy of Orthapaedic Surgeons. OrthoInfo: Metastatic Bone Disease. https://orthoinfo.aaos.org/en/diseases–conditions/metastatic-bone-disease/ Accessed October 19, 2020.
- Wisanuyotin, T et al. Prognostic and risk factors in patients with metastatic bone disease of an upper extremity. Journal of Bone Oncology. 2018 Nov; (13): 71-75. https://doi.org/10.1016/j.jbo.2018.09.007.
- Janjan, Nora et al. Pathological Fracture. Science Direct. https://www.sciencedirect.com/topics/medicine-and-dentistry/pathologic-fracture. Accessed October 19, 2020.
- American Cancer Society. Bone Metastases. https://www.cancer.org/treatment/understanding-your-diagnosis/advanced-cancer/bone-metastases.html. Accessed October 6, 2020.
- John Hopkins Medicine. Conditions and Diseases: Spinal Cord Compression. https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-cord-compression. Accessed October 6, 2020.
- Gralow, Julie et al. National Comprehensive Cancer Network. NCCN Task Force Report: Bone Health in Cancer Care. Journal of National Comprehensive Care Network. https://www.nccn.org/JNCCN/PDF/2009_Bone_Health_TF.pdf. Accessed October 6, 2020.
- Mayo Clinic. Osteoporosis treatment: Medications Can Help. https://www.mayoclinic.org/diseases-conditions/osteoporosis/in-depth/osteoporosis-treatment/art-20046869. Accessed October 6, 2020.
Putting the Power in Hands of the Underserved
To recruit Black women in clinical trials, we need to educate communities and say, okay, we know about the Tuskegee project and we can add a lot about the different projects. But there are things in place that hopefully prevent hospitals, oncologists, and researchers from having that same history. -Sheila Marie McGlown
Nunny Keyla Reece was diagnosed with ER/PR and HER2 metastatic breast cancer in 2017.
After finding a lump in her breast in 2015, and receiving a mammogram, the radiologist told Nunny it was benign fatty tissue and to return if she noticed any changes. She was 37 at the time, with no history of breast cancer in her family. In 2017, she started to have severe pain in her back and at the same time, she found a new lump under her arm. At 39, she was diagnosed with metastatic breast cancer (mbC). “All I could think about,” she says, “was my husband and children.”
Nunny began to attend conferences to educate herself. She also started sharing her own story to educate her community. When she was first diagnosed, she felt alone. This was because at first she did not encounter other Black women with mBC. But according to Nunny, the problem runs deeper than that. Black women do not see Black women included in commercials or magazines, at conferences or in brochures. For this reason, “they think mBC is only a white woman disease. This is unacceptable.” The lack of representation in media and in the medical community’s outward facing educational materials leads to disparities in prevention and treatment. And it reflects the lack of inclusion of Black women in research and the development of medical advancements.
Many Black women also lack equal access to care and treatment that can improve quality of life and extend life. Nunny has experienced this firsthand in the system and in her relationships with medical professionals, starting with the radiologist’s incorrect diagnosis in 2015, and extending to relationships with her physicians.
“You want to trust your physician,” Nunny Keyla Reece says, “whether you’re Black or white.” But racism exists everywhere: work, school, and the doctor’s office. And when living with mBC, it’s hard if you can’t get the care you need. In the past, she noticed that white friends received information about chemotherapy or clinical trials. When Nunny asked about these options, physicians would tell her, “You don’t have anything to worry about.” And they did not listen and respond to her concerns. When Nunny complained of having headaches for the first time, her physician said it was probably allergies. She had to argue for tests. “To completely shut someone down, especially when you are already in stage IV,” Nunny says, “Why would someone do that? It’s not putting my care first.” When she received MRI results showing a brain mass, Nunny was glad she spoke up and caught it in time.
When Nunny heard other Black women speak about similar experiences, she realized it happened to them, too. “Sometimes the care level is just different,” she explains. She does not want a doctor who will not give it their all, who will “give up before I’m giving up.” So far she has shifted through four physicians, seeking what she needs: a physician who cares about her as a human being and will try to build a bridge to mutual understanding, someone who will open a space to learn about her and ask the right questions. She needs a physician who will explain what she should know and do; and answer her questions fully. Nunny will do whatever it takes and she expects the same from her physicians.
Bio:
Nunny Keyla Reece, a former certified medical assistant in pain management, is an Angel Advocate with the Tigerlily Foundation and works to reduce racial health disparities. She believes passionately that it is important for people with mBC to be able to express themselves freely in the support of a community, and advocate for what they need in the medical community, which includes both empathy and access to the best care. Nunny works to pay forward the support she has received, and to love life with her family and broader community.
Being Catapulted into a New Frontier: Moving from Challenge to Catalyst
This video has been brought to you by the #MyLifeIsMyLegacy Campaign
“My story with breast cancer can be seen as tragic. But instead, I want people to see it as hopeful and inspiring. I’m still a dynamic, loving 37 year-old woman. And at every moment since my diagnosis, I am still LIVING. Cancer is part of my life but it doesn’t define me.” -Julia Maues
Cancer is traumatic, painful, catastrophic, and life-altering. The trauma of breast cancer occurs not only from the cancer itself, but also from the treatment and from navigating the medical system. It can also be traumatic to witness suffering and experience the loss of others. Along the way, some experiences may heighten the trauma. Other experiences, like having community support, or a spiritual awakening, can strengthen us, give us a new perspective, and even motivate us to take action.
When you receive an initial diagnosis of cancer, you may experience a range of emotions, including shock, fear, grief, confusion, exhaustion, desperation, hopelessness, anger, rage, or doubt. When Nunny Keyla Reece first found out she has metastatic breast cancer (mBC), she woke up every morning wondering, “Am I going to die today . . . ?” She felt fear and often cried when she felt anything new happening with her body. She would think, “Is this it?” The unknown worsened her fear because she didn’t understand what was happening. She had anxiety attacks for the first time in her life.
Similarly, Jamil Rivers describes her first moments of mBC as being “catapulted into a whole new frontier of everything.” She felt afraid that she would not be able to see her sons grow up or grow old with her husband. Yet no state is permanent. Over time, what became most traumatic for Jamil was the loss of those with whom she developed close relationships. Of those she lost, Jamil explains, “They were diagnosed before me and they’re just as passionate. They tried to push through and they ran out of time. Now I have to keep that work going. I’m looking at my time that I have left and trying to make the most of it.”
Your feelings might also shift, day to day and over time. Sheila Marie McGlown explains that when she was diagnosed with mBC at 43, she saw her life in “fast forward; I thought about when I was born to up to the age of 43.” She thought, “Where did it go?” She struggled to accept the cancer until one one morning when she woke up and noticed her hair on the bed. In that moment, she experienced a radical shift. “I have no control over this,” she thought, and that was when she accepted the it. After learning of estimated survival rates, Sheila made a bucket list so that she could make every moment count. Then after year 5, she thought, “hhmm. I’m not dead yet.” And after year 6, she thought, “hhmm.” And a decade later, she thinks, ”I’M STILL HERE.”
Eventually, you might move from the initial shock to a place of acceptance where the unexpected can occur. Alongside the trauma of cancer, many develop what is called posttraumatic growth, which is personal development or “positive change” that results from “struggle with a major life crisis or a traumatic event.” This does not happen overnight; it’s gradual and happens in fits and starts. You may experience moments of this right now; it’s also okay to not feel this way at all.
If and when you experience posttraumatic growth, you may develop a sense that the struggle gives you newfound purpose or opportunities. You might experience a newfound closeness with others or connection to people who suffer from cancer or other traumas. You may develop an awareness of your own strength and “appreciation for life in general.” You may also develop a deepening of spiritual life and a shift in priorities (Posttraumatic Growth Research Group). As Nunny explains, “I didn’t want to live my life being scared, so I changed my whole life. I started deepening my spiritual relationship with God and without that, it would have been so hard for me.”
Julia Maues was diagnosed with breast cancer in 2013, while pregnant. “To my surprise,” she says, “chemo during pregnancy is the standard of care. I delivered a healthy baby boy with a head full of hair while I had no hair at all.” After her son was born, Julia did tests she could not do while pregnant, and learned that the cancer had spread to her brain, liver, and bones. After trying different drugs and finding the right one, the cancer started to respond to the therapy. Julia continues to experience many setbacks. As she explains, “Most drugs don’t penetrate the brain, many drugs harm the heart, the side effects can be debilitating, and my illness has taken a huge emotional toll on me and my loved ones.” But she still expresses the most authentic parts of herself: “I’m still a dynamic, loving 375-year-old woman. And at every moment since my diagnosis, I am still LIVING. Cancer is part of my life but it doesn’t define me.”
Julia’s experience also opened her eyes to inequities in breast cancer research and treatment. “Did you know that the share of the money obtained in pink campaigns that goes to research on metastatic breast cancer is negligible compared to where the rest of the money goes? Or that breast cancer mortality is 40 percent higher for Black women? Metastatic breast cancer is the only breast cancer that kills and research is the only effort that truly helps patients do what we want to do – LIVE! That is not pink!”
Since developing this awareness, Julia has become involved in advocacy, which has been rewarding. She says that she enjoys connecting with researchers and “showing them the side of breast cancer they often can only imagine – the life of a patient.” After recently collaborating with a researcher, he told her, “‘Regardless of whether we meet again, I want you to know I have been moved by your profound fighting spirit and it is making me redouble my efforts within my research.’” During her lifetime, Julia’s goal, like that of so many advocates with mBC, is “to make an impact in the lives of others dealing with this disease.”
Jamil Rivers -Putting the Power in the Hands of Black Women
This video has been brought to you by the #MyLifeIsMyLegacy Campaign
Jamil Rivers was diagnosed with mBC in 2018 at the age of 39. As a mother of three, caregiver, and working professional, Jamil has a fierce determination to survive. She has learned a lot about life and herself through her struggles with mBC. For one thing, she knows that she’s strong and can make a positive difference. In her first year of chemotherapy, Jamil worked her first year of a new job. Worried about the possibility of losing her job (including income and benefits), she did not disclose her diagnosis at work. She shaved and tattooed her eyebrows, wore a wig, and went to work and chemotherapy every day. Fortunately for Jamil, her treatments were showing positive results and her tumors were shrinking. Now on an oral treatment, she is focused on living her best life and leading as an advocate for other Black women who may face inequalities and disparities in the medical system. Before her cancer diagnosis, she says, “I never questioned God’s path for me.” Yet when she received her diagnosis, it immediately followed her husband’s recent recovery from cancer. And so at first, she thought, “My kids already have one parent with cancer. Now you’re going to give them two parents with cancer?” But eventually, she realized, “Well, why not me. Cancer focuses your life. It clears out everything that’s not important. It educates you about who you are. I’m stronger than what I ever believed possible and I have accomplished more than I ever thought possible.”
In response to mBC, Jamil became motivated to survive for her family and become an advocate for change. Jamil believes that the most violent aspect of cancer is the unequal medical system and unjust racial health disparities that prohibit treatment and worsen cancer outcomes for many Black women. This is the most violent aspect of cancer because of Black women’s vulnerability to “a system with unconscious bias and structural racism.” This bias can impact care with devastating effects. But if Jamil can make a difference in “penetrating people’s thoughts, emotions, and motivations in order for us to really get to the crux of the problem, then, okay.”
In addition to her own work, Jamil has also seen growth in her children. She explains that they also express learning and becoming motivated from their parents’ experiences with cancer. “I see my kids growing into these empathetic, compassionate, intelligent, thoughtful, curious people,” she says, “and they’re amazing human beings.” Of cancer, Jamil says, “I never believed that cancer is a gift,” but it’s a crucial “part of my story.” Even though it is horrible and scary, Jamil accepts it. “I’m still here,” she says. “I’m still breathing. So I’m going to live my life and do what I can with this.”
Bio:
Jamil Rivers, who was raised in New Jersey and now lives in suburban Philly, is married to the love of her life and has three amazing boys. Jamil and her husband are both cancer survivors and have both been caregivers and patients at different times. Jamil is close to her family, sisters, and girlfriends, loves crossword puzzles, and describes herself as a foodie. She also works full time as Chief Financial Officer of Education Works; is Board President of Metavivor Research and Support, Inc.; a Board member of Living Beyond Breast Cancer; and an Angel Advocate with the Tigerlily Foundation. Jamil also founded a breast cancer education and navigation organization called The Chrysalis Initiative.
Talking about mBC Saves Lives
Bridging the Gap Between Early-Stagers and Metastatic Breast Cancer
“Not everything that is faced can be changed, but nothing can be changed until it is faced.” -James Baldwin, “As Much Truth As One Can Bear,” The New York Times, January 14, 1962
Alongside other warriors, as a 14-year survivor, Maimah dedicates her life to advocating for improvements to education and treatments needed to make mBC a chronic disease, not a terminal one. To do this, it is crucial for every person to realize their value and importance in this mission, and that they are a hero in their own life as well as in the lives of others. When we commit to something greater than ourselves, we realize and experience what this truly means.
If more people talk about mBC, as a society, we can save more lives. And it’s important for those with mBC to participate in and lead those conversations. The more opportunities for others to hear from those with mBC, the more others will connect and find resonance. As Jamil explains, “I do think that connection does have to happen where it resonates. And I think that’s with everything in history. When you are living, breathing and, you know, fraternizing with people that are not like yourself, it expands your thoughts, opinions, and understanding.” Many people do not realize that people can die from breast cancer and that with access to appropriate care, people with mBC can live a high quality of life for a long time. Jamil explains that when people connect with her story, this motivates them to learn and advocate for solutions. If we keep the conversation going, this may lead to more investment in funding for research about mBC, which leads to advances that improve diagnosis and treatment for mBC as a chronic disease. As Jamil argues, “Let’s address mBC, so that we can disrupt the entire process and save lives.”
Every person is touched by breast cancer, whether it is you or someone you know and love. Watch videos and read stories of the My Life is My Legacy campaign to witness how many people—early stagers, those with mBC, caregivers, doctors, and researchers—live their lives as legacies and work for a better future for those living with mBC. Learn how you can do the same.
This article is a part of the #MyLifeIsMyLegacy Campaign. Learn more here.